ABOUT ASCENIVTM
Study 1 Design: A 52-week, prospective, open-label, nonrandomized, multicenter, phase 3 study that evaluated the efficacy and safety of ASCENIV in patients with PI (N=59). Intravenous infusions were administered at doses of 300 to 800 mg/kg every 3 or 4 weeks. There were 19 subjects with a 3-week cycle and 40 subjects with a 4-week cycle. There were 45 subjects (76%) with common variable immunodeficiency (CVID) as their primary diagnosis, followed by X-linked agammaglobulinemia (10%), antibody deficiencies and "other" (7% each). The modified intent-to-treat (mITT) population included 59 subjects and was used for efficacy analysis. Primary efficacy endpoint was the demonstration of an acute serious bacterial infection (SBI) rate of <1.0 per person-year during the 52-week treatment period. Secondary efficacy endpoints included number of missed days of work/school/activity due to infection, unscheduled visits to the physician, and days hospitalized because of infection.1,5
Study 2 (Pediatric Study) Design: A 6-month prospective, open-label, nonrandomized, multicenter study evaluated the efficacy and safety of ASCENIV in pediatric patients with PI (N=16). Intravenous infusions were administered at doses of 300 to 800 mg/kg every 3 or 4 weeks (based on the dose and schedule of their prior treatment regimen) for approximately 5 months. In the overall study population (N=16), the most common PI diagnosis was hypogammaglobulinemia (50.0%), followed by CVID (25.0%), X-linked agammaglobulinemia (12.5%), and selective polysaccharide antibody deficiency (also known as specific antibody deficiency) (12.5%). The primary efficacy measure was the rate of SBIs. The predefined success criteria was demonstration of rate of less than one acute SBI per patient per year. No acute SBIs occurred during the 6-month observation period, yielding a mean number of acute SBI episodes per person-year of 0.0. No other serious infections, or hospitalizations due to infections occurred.1,5
HOW ASCENIV IS MADE
Learn how ASCENIV is manufactured using patented methodologies for donor screening and plasma pooling1*
ASCENIV—the only IVIG produced from blending RSV plasma with normal source plasma1*
PLASMA COLLECTION AND SCREENING
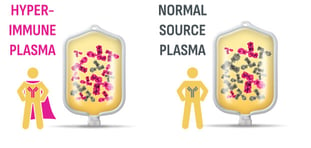
- Hyperimmune donors with RSV antibodies are identified using ADMA’s proprietary screening technology2,3
- These donors are associated with increased titers for 8 other common respiratory viruses3,4
- Plasma is collected from US FDA-licensed plasma collection centers2
TESTING
- Proprietary microneutralization assay quantifies levels of neutralizing antibodies in hyperimmune plasma donor samples2
TAILORED POOLING
ASCENIV is the only IVIG product available that is manufactured using patented methodologies for donor screening and plasma pooling*
- Normal source plasma is blended with RSV plasma to produce a tailored plasma pool derived from a minimum of 1,000 unique donors2,5
- Meets potency requirements for 21CFR6403
*ADMA BIOLOGICS PATENTS ISSUED 9,107,906, 9,714,283, 9,815,886, 9,969,793, 10,683,343, 11,339,206, 11,780,906, 12,473,351.
FDA=US Food and Drug Administration; IgG=immunoglobulin G.
ASCENIV provides a broad spectrum of neutralizing IgG
antibodies against bacterial and viral pathogens and their toxins5
Expert Insights
Dr. Kelli Williams, MD, MPH shares insights from her long-term experience with ASCENIV, highlighting its benefits and the real-world impact it has had on her patients managing Primary Immunodeficiency.
Efficacy
Inside ASCENIV—efficacy to prevent serious infections5
In two, prospective, open-label, multicenter, nonrandomized studies evaluating the efficacy and safety of ASCENIV in adult in pediatric patients with PI 5:
With the proven protection of ASCENIV, reduce infection-related quality-of-life impact, so your patients can focus on what counts5
Efficacy results (PPPY) in the 1-year study (secondary endpoints):
0
hospitalizations due to infection5
One patient from the study group was hospitalized because of a postoperative local wound infection from elective surgery5
<1
unscheduled medical visit PPPY5
24 out of 59 patients (41%) had a total of 54 unscheduled medical visits due to infections5
1.7
missed days of work/school/
activity PPPY due to infection5
23 patients (39%) had a total of 93 missed days of work/school/activity due to infections out of a total of 20,417 patient days (<0.5%)5
32.9
days of antibiotic use PPPY5
37 patients (63%) used antibiotics due to infection (includes therapeutic use)5
*SBIs were defined as a rate of <1.0 cases of bacterial pneumonia, bacteremia/septicemia, osteomyelitis/septic arthritis, visceral abscess, and bacterial meningitis per person-year.5
PPPY=per patient per year.
Quality
ADMA is committed to excellence when producing specialty biologics designed to safely and effectively treat the immunocompromised1
ADMA has created a robust, sustainable, reproducible, and controlled supply and production process for ASCENIV1


Focused on what counts: safety, quality, and efficacy
Dosing, Administration, and Storage
ASCENIV dosing, administration, and storage5
For adults and pediatric patients (2 years of age and older) with PI5
For intravenous use only
Dose
300 to 800 mg/kg every 3 to 4 weeks*
*Frequency/amount of IgG therapy may vary from patient to patient. The proper amount can be determined by monitoring clinical response.
Initial infusion rate
(for first 15 minutes)
(for first 15 minutes)
0.5 mg/kg/min
(0.005 mL/kg/min)
Maintenance infusion rate (if tolerated)
Increase gradually every 15 minutes up to 8 mg/kg/min (0.08 mL/kg/min)
- No apparent differences in efficacy or safety between 3- and 4-week dosing5
- The dose may be adjusted over time to achieve the desired trough levels and clinical response5
- ASCENIV dose adjustments may be required in patients who fail to maintain trough total IgG concentrations of at least 500 mg/dL with a target of 600 mg/dL. Starting with the second infusion, adjust the dose proportionally, targeting a trough of ≥600 mg/dL, based on the previous trough and the associated dose5
ASCENIV is a liquid solution containing 10% IgG (100 mg/mL) for intravenous infusion5
- Available in a single-use non-latex, tamper-evident 5g/50 mL vial with a hanger label5
- Begin with an initial infusion rate of 0.5 mg/kg/min. If there are no adverse reactions, the infusion rate for subsequent infusions can be slowly increased to the maximum rate5
- Monitor patient vital signs throughout the infusion. Slow or stop the infusion if adverse reactions occur. If symptoms subside promptly, the infusion may be resumed at a slower rate that is comfortable for the patient5
- Ensure that patients with preexisting renal insufficiency are not volume-depleted. For patients judged to be at risk for renal dysfunction or thrombotic events, administer ASCENIV at the minimum infusion rate practicable, and consider discontinuation of administration if renal function deteriorates5

Storage5
- Once vial is entered, use promptly5
- Store at 2-8 °C (36-46 °F) for up to 36 months from the date of manufacture5
- Do not freeze5
- Product may be stored up to 4 weeks at ≤25 °C (77 °F). After storage at room temperature product must be used or discarded5

The ASCENIV Dosing and Administration Guide
Find detailed instructions on how to dose and administer ASCENIV in this guide.

Safety
ASCENIV — a demonstrated safety profile5
- In Study 1, 59 patients with PI received a total of 793 infusions of ASCENIV at a median dose of 505 mg/kg (range 284 to 1008 mg/kg) every 3 weeks or 4 weeks for up to 12 months (mean 346 days; range 36 to 385 days). Of the 793 infusions administered during this trial, 7 (11.9%) patients received premedication prior to 7 (0.9%) infusions5
- The most common adverse reactions occurring in ≥5% of patients in Study 1 are presented below
Adverse Reactions (within 72 hours after the end of an ASCENIV infusion) in ≥5% of subjects
Adverse Reactions |
Number (%) of Subjects (N=59) |
Number (%) of Infusions (N=793) |
|---|---|---|
| Headache | 14 (24) | 21 (2.6) |
| Sinusitis | 6 (10) | 7 (0.9) |
| Nausea | 5 (9) | 5 (0.6) |
| Acute sinusitis | 4 (7) | 4 (0.5) |
| Fatigue | 4 (7) | 9 (1.1) |
| Muscle spasms | 4 (7) | 4 (0.5) |
| Bronchitis | 3 (5) | 3 (0.4) |
| Diarrhea | 3 (5) | 3 (0.4) |
| Epistaxis | 3 (5) | 4 (0.5) |
| Muscle pain | 3 (5) | 5 (0.6) |
| Oropharyngeal pain | 3 (5) | 3 (0.4) |
| Pain in extremity | 3 (5) | 3 (0.4) |
| Itching | 3 (5) | 3 (0.4) |
- In Study 2 (pediatric study), 16 pediatric patients with PI aged 2 to 11 years received 91 infusions of ASCENIV at a median dose of 541 mg/kg (range 300-800 mg/kg) every 3 or 4 weeks for approximately 5 months5
- The most common adverse reactions occurring in ≥5% of patients in Study 2 are presented below
Adverse Reactions (within 72 hours after the end of an ASCENIV infusion) in ≥5% of subjects
Adverse Reactions |
Number (%) of Patients (N=16) |
Number (%) of Infusions (N=91) |
|---|---|---|
| Chest Pain | 1 (6) | 1 (1) |
| Epistaxis | 1 (6) | 1 (1) |
| Fatigue | 1 (6) | 1 (1) |
| Hypersensitivity | 1 (6) | 1 (1) |
| Diarrhea | 1 (6) | 1 (1) |
| Headache** | 4 (25) | 5 (5) |
| Otitis** | 2 (13) | 2 (2) |
| Viral Rash | 1 (6) | 1 (1) |
| Vomiting | 1 (6) | 1 (1) |
| Nausea | 3 (19) | 4 (4) |
| **Includes multiple related terms. | ||
Product Characteristics
Product characteristics5
- ASCENIV is a liquid solution containing 10% IgG (100 mg/mL) for intravenous infusion5
- The broad spectrum of neutralizing IgG antibodies against bacterial and viral pathogens and their toxins helps to avoid recurrent serious opportunistic infections5
- Purified, sterile, ready-to-use preparation5
- Clear to opalescent liquid (colorless to pale yellow)5
- Normal IgG subclass distribution5
- Formulated in water for injection containing 0.100 M-0.140 M sodium chloride, 0.20 M-0.29 M glycine, 0.15%-0.25% polysorbate 80, and pH 4.0-4.6. Contains no sucrose5
- Contains ≤200 μg/mL of immunoglobulin A5
- Mean half-life of ASCENIV5:
- 28.5 ± 4.4 days for patients on a 3-week dosing regimen
- 39.7 ± 11.6 days for patients on a 4-week dosing regimen
The only IVIG available that is manufactured using ADMA Biologics’ patented methodologies for donor screening and plasma pooling.*

Size of vial not to scale.
Available in a single-use non-latex, tamper-evident 5g/50 mL vial with a hanger label5
*ADMA BIOLOGICS PATENTS ISSUED 9,107,906, 9,714,283, 9,815,886, 9,969,793, 10,683,343, 11,339,206, 11,780,906, 12,473,351.
Indication
ASCENIV™ (immune globulin intravenous, human–slra) is a 10% immune globulin liquid for intravenous injection, indicated for the treatment of primary humoral immunodeficiency (PI) in adults and pediatric patients (2 years of age and older). PI includes, but is not limited to, the humoral immune defect in congenital agammaglobulinemia, common variable immunodeficiency (CVID), X linked agammaglobulinemia, Wiskott-Aldrich syndrome, and severe combined immunodeficiencies (SCID).
Important Safety Information for ASCENIV
WARNING: THROMBOSIS, RENAL DYSFUNCTION AND ACUTE RENAL FAILURE
- Thrombosis may occur with immune globulin intravenous (IGIV) products, including ASCENIV. Risk factors may include: advanced age, prolonged immobilization, hypercoagulable conditions, history of venous or arterial thrombosis, use of estrogens, indwelling vascular catheters, hyperviscosity, and cardiovascular risk factors.
- Renal dysfunction, acute renal failure, osmotic nephrosis, and death may occur with the administration of IGIV products in predisposed patients. Such events require immediate medical intervention, if not recognized or managed appropriately, may result in persistent or significant disability or lead to fatal outcome.
- For patients at risk of thrombosis, renal dysfunction or renal failure, administer ASCENIV at the minimum dose and infusion rate practicable. Ensure adequate hydration in patients before administration. Monitor for signs and symptoms of thrombosis and assess blood viscosity in patients at risk for hyperviscosity.
Contraindications
ASCENIV is contraindicated in:
- Patients who have had an anaphylactic or severe systemic reaction to the administration of human immune globulin.
- IgA-deficient patients with antibodies to IgA and a history of hypersensitivity.
Warnings and Precautions
Severe hypersensitivity reactions may occur with IGIV products, including ASCENIV. In case of hypersensitivity, discontinue ASCENIV infusion immediately and institute appropriate treatment. Medications such as epinephrine should be available for treatment of acute hypersensitivity reactions. Patients with known antibodies to IgA may have a greater risk of developing severe hypersensitivity and anaphylactic reactions.
Thrombosis may occur following treatment with immune globulin products, including ASCENIV, and in the absence of known risk factors. Consider baseline assessment of blood viscosity in patients at risk for hyperviscosity and ensure adequate hydration before administration. For patients at risk of thrombosis, administer ASCENIV at the minimum dose and infusion rate practicable. Monitor for signs and symptoms of thrombosis and assess blood viscosity in patients at risk for hyperviscosity.
Acute renal dysfunction, acute renal failure, acute tubular necrosis, proximal tubular nephropathy, osmotic nephrosis, and death may occur upon use of human IGIV products. Ensure that patients are not volume depleted before administering ASCENIV. Periodic monitoring of renal function and urine output is particularly important in patients at increased risk of developing acute renal failure. Assess renal function, including measurement of blood urea nitrogen (BUN) and serum creatinine, before the initial infusion of ASCENIV and at appropriate intervals thereafter. Discontinue ASCENIV if renal function deteriorates. In at risk patients, administer ASCENIV at the minimum infusion rate practicable.
Hyperproteinemia, hyperviscosity, and hyponatremia may occur in patients receiving IGIV treatment, including ASCENIV. It is critical to clinically distinguish true hyponatremia from a pseudohyponatremia that is associated with or causally related to hyperproteinemia. Treatment aimed at decreasing serum free water in patients with pseudohyponatremia may lead to volume depletion, a further increase in serum viscosity, and a possible predisposition to thrombotic events.
Aseptic meningitis syndrome (AMS) may occur with IGIV treatments, including ASCENIV. AMS usually begins within several hours to 2 days following IGIV treatment. The risk of AMS may be higher with high doses (≥2 g/kg) and/or rapid infusion of IGIV. Conduct a thorough neurological examination on patients exhibiting signs and symptoms of AMS, including cerebrospinal fluid (CSF) studies, to rule out other causes of meningitis. Discontinuation of IGIV treatment has resulted in remission of AMS within several days without sequelae.
Hemolysis may occur after administration of IGIV products, including ASCENIV, due to the presence of blood group antibodies that can act as hemolysins and induce in vivo coating of red blood cells (RBCs) with immunoglobulin, causing a positive direct antiglobulin test and hemolysis. The risk factors for hemolysis include high doses (e.g., ≥2 g/kg) given either as a single administration or divided over several days, non-O blood group, and an underlying inflammatory disease condition. Monitor patients for clinical signs and symptoms of hemolysis, including appropriate confirmatory laboratory testing.
Transfusion-Related Acute Lung Injury (TRALI) may occur in patients following IGIV treatment, including ASCENIV. Monitor patients for pulmonary adverse reactions. If TRALI is suspected immediately stop ASCENIV infusion and perform appropriate tests for presence of anti-neutrophil antibodies and anti-human leukocyte (HLA) antibodies in both product and patient’s serum. Manage patients using oxygen therapy with adequate ventilatory support as appropriate.
There is risk of transmitting infectious agents including viruses, the variant Creutzfeldt-Jakob disease (vCJD) and the Creutzfeldt-Jakob disease (CJD) agent with ASCENIV administration because it is manufactured using human blood. All infections suspected to have been transmitted by ASCENIV should be reported by the physician or other healthcare provider to ADMA Biologics at (1-800-458-4244).
After infusion of immunoglobulin, the transitory rise of the various passively transferred antibodies in the patient’s blood may yield positive serological testing results, with the potential for misleading interpretation. Passive transmission of antibodies to erythrocyte antigens (e.g., A, B, and D) may cause a positive direct or indirect antiglobulin (Coombs’) test.
Adverse Reactions
The most common adverse reactions to ASCENIV (≥5% of study patients) were headache, nausea, otitis, sinusitis, fatigue, chest pain, muscle spasm, acute sinusitis, diarrhea, hypersensitivity, viral rash, vomiting, bronchitis, epistaxis, muscle pain, oropharyngeal pain, pain in extremity and itching.
To report SUSPECTED ADVERSE REACTIONS, contact ADMA Biologics at (1-800-458-4244) or FDA at 1-800-FDA-1088 or www.fda.gov/MedWatch. For additional safety information about ASCENIV, please see full Prescribing Information.